https://blog.priceplow.com/podcast/dr-cameron-sepah-maximus-062
On February 2, 2022, we hosted Dr. Cameron Sepah of Maximus on the PricePlow Podcast to talk about male hormones and self improvement. This was an incredible episode covering a wide variety of health-based topics, and everyone is sure to come away with some new knowledge.
Meet Dr. Cameron Sepah
Meet Dr. Cameron Sepah, founder of Maximus, whose here to help you boost testosterone in a clinically-meaningful way without TRT. Prepare to learn a ton about enclomiphene in this episode!
Cam, as we call him, competed as a track athlete. is a clinical psychologist, with a fellowship training in behavioral medicine, working at the intersection of psychology and medicine. He competed as a collegiate track athlete, racing in mid-distance to distance events. After his academic training (specializing in psychoneuroendocrinology amongst other fields) and publishing of several papers,[1] he created Omada Health, an online weight loss program. All in all, he's a clinician-scientist who's treated people for over a decade. In addition, he's an assistant clinical professor of psychiatry at the UCSF School of Medicine.
Maximus: Mind, Body, and Masculinity
Cam recently founded Maximus, a consumer telemedicine company for men's health and hormone optimization. Using at-home blood testing and online coaching, Maximus has put together the King Protocol, which is a clinically-validated process to safely increase testosterone and vitality in men - even healthy and young men.
This is not testosterone replacement therapy -- it's testosterone restoration.
Prepare to learn about enclomiphene citrate
Jumping right to hormone optimization, Maximus utilizes enclomiphene citrate -- the isomer from clomid that's safer and more useful in men -- to meaningfully boost testosterone levels anywhere from 1.5x to 2.5x. Combined with group health coaching for nutrition, exercise, sleep, and focus, alongside some adjunct supplements, Maximus is changing men's lives at an astonishing rate.
The full show notes with timestamps are covered below - and we have a separate article detailing enclomiphene citrate.
![]()
Audio Version:
Podcast: Play in new window | Download (Duration: 1:38:56 — 87.7MB)
Subscribe to the PricePlow Podcast on Your Favorite Service (RSS)
Apple Podcasts

Spotify

YouTube
Our Discussion with Dr. Cameron Sepah of Maximus
-
0:45 - Dr. Cam's Introduction
-
2:50 - A couple of Dr. Cam's legendary Twitter threads:
-
Clinical experience: most people struggle because their main motivations are inverted - but Cam explains how he helps change that:
https://twitter.com/DrCamRx/status/1100058665774592001 -
"If I could only pick two psychological techniques to transform yourself":
https://twitter.com/DrCamRx/status/1180205914973818880 -
Six Healthy Eating Rules:
https://twitter.com/DrCamRx/status/1237785720158224384 -
Secret to high performance is managing stress:
https://twitter.com/DrCamMaximus/status/1455335722920013825 -
Nature provides the best free health:
https://twitter.com/DrCamRx/status/1174453771037855745
-
-
3:50 - Dr. Cam's Background in medicine and psychiatry
Became interested in the hormone side of health. Psychiatry took a very "neurotransmitter approach" - for instance, SSRIs are based on an "almost stupidly simplistic theory" of the monamine hypothesis, even though the research hasn't fully supported that, and it's more complicated than serotonin - it's really a "bio-psycho-social phenomenon". Hormones also influence brain function!
-
4:45 - The problem: Human testosterone and sperm levels are tanking
Testosterone levels have declined 50% over 50 years[2] and so have sperm counts.[3-6] The question is why?! This is a dramatic phenomenon - it's happened over a couple of generations, alongside the obesity epidemic.

Due to an onslaught of endocrine-disruptions, men's hormonal systems aren't working like they used to. Maximus has a three-pronged solution called the KING Protocol. Image courtesy Maximus.
-
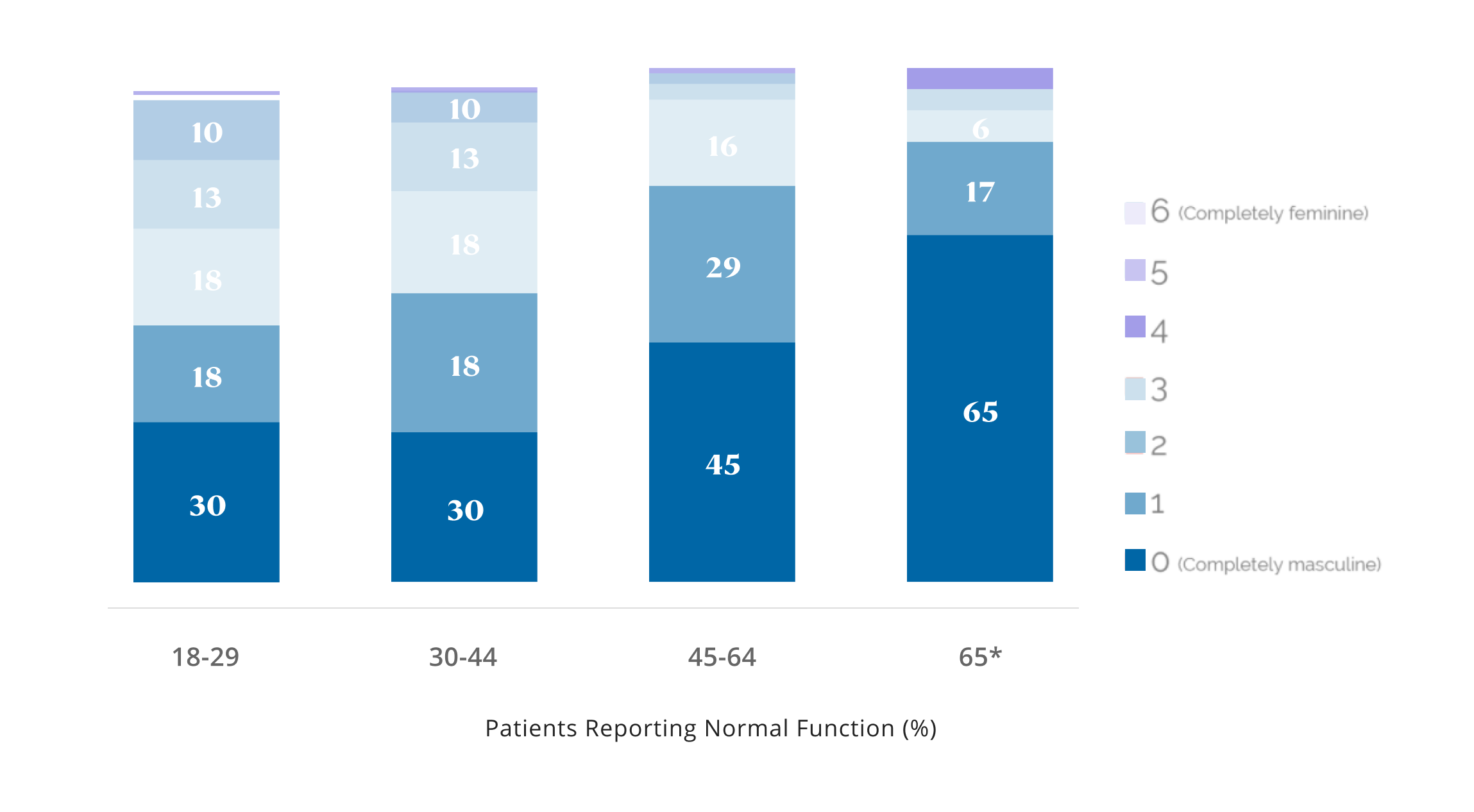
5:45 - Body fat is one culprit... but not the only one
Body fat -- the extra belly fat in particular -- has the aromatase enzyme in it, converting testosterone to estradiol. The more body fat you have, the less masculine and more feminine you become. But even adjusting for obesity and increased depression, testosterone and sperm are still going down! There's something more than just obesity causing these issues.
-
6:45 - Endocrine-disrupting chemicals
Endocrine-disrupting chemicals are in everything - the water we drink (note from Mike: consider the famous atrazine frog study[8]), plastics on our foods that release microplastics, teflon non-stick pans and air fryers, plastic bottled water (they've gotten rid of BPA but not BPS), etc. These are xenoestrogens -- they mimic estrogens in the body and disrupt the endocrine system.
-
7:45 - It's happening to dogs too!
Sperm count is even going down in dogs[9] - they're drinking the same water and eating the same processed food as us. That adds evidence that it's environmental. Forbes: You're not the man your father was.[10] He wasn't eating 66%-84% of his food from processed food like we do.[11]
-
9:20 - "We essentially have a hormonal handicap these days - and it's the public health tragedy that no one's talking about"
-
9:45 - Mike: polyester clothing and synthetic fabrics are a vastly underrated endocrine disruptor
Mike briefly also adds in the contributions from polyester clothing, something he's been researching that looks extraordinarily devastating - especially if worn as underwear.[12-16] Digging into those studies, we'll definitely need to cover this in greater detail later on.
-
10:15 - ACTION Plan - Where do we begin?
-
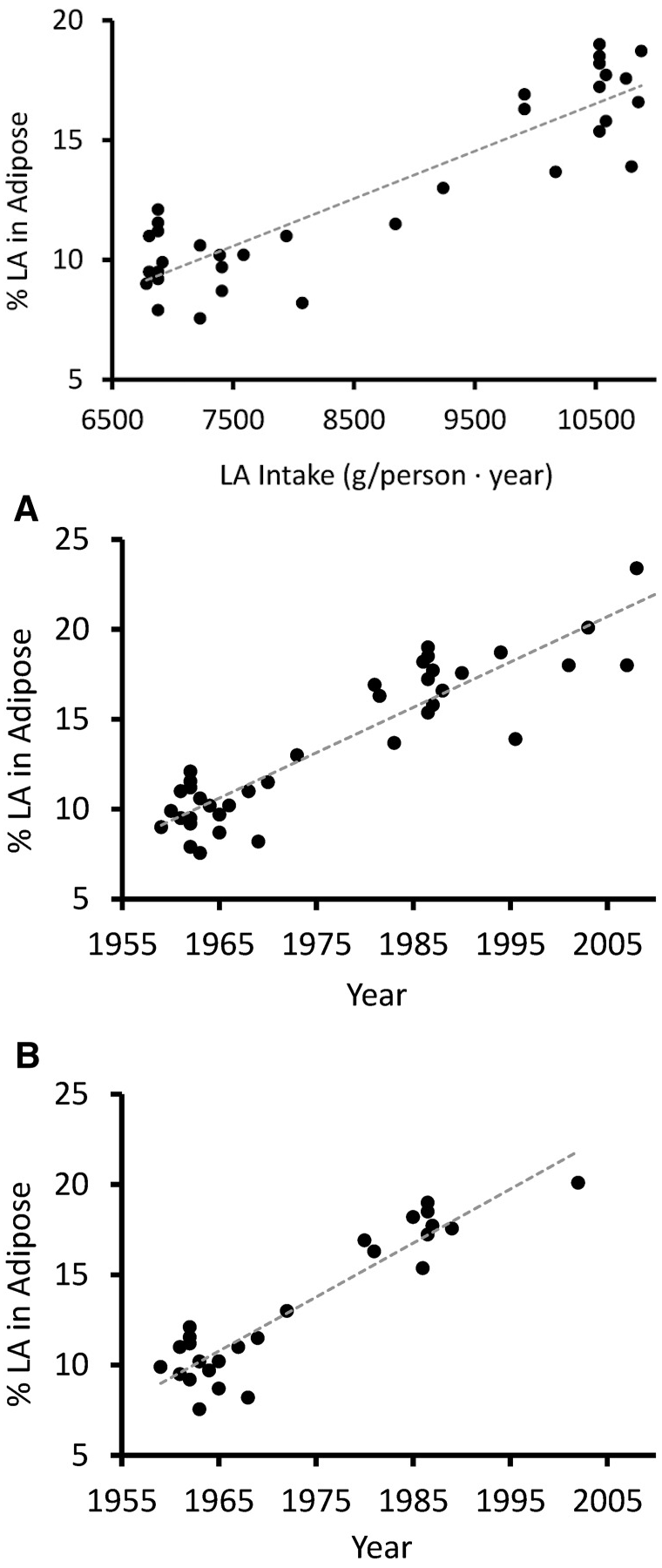
Maintaining a healthy level of body fat

Increased Linoleic Acid Consumption... Increased Linoleic Acid bodyfat Composition[7]... increased obesity. We believe that this omega-6 fatty acid, coming mostly from industrialized processed seed oils, is the most major culprit in the obesity crisis.
15% (slightly visible abs) is a good place to get to and achievable naturally. Don't need to be single-digits. Remove as many ultra-processed foods as possible, don't kill yourself over getting rid of 100% processed food though -- read The Cure for Obesity and Diabetes Is Processed Food Parts 1, 2, and 3.[17-19]
Ancestral processed food like yogurt and butter is fine - but a Cheeto is not. Be selective of processed foods, they should be the minority, not the majority.
-
Reasonably avoid plastics
Avoiding plastics doesn't need to make you OCD. Drink filtered water, preferably from reverse osmosis filtration. Don't keep stuff in plastics - try to use steel and glass to store your food. Cook in cast iron, not teflon pans.
-
Fight fire with fire
You can do things pharmacologically to combat the chemical onslaught we face to get your testosterone back to ancestral levels. This is where Maximus is heading, so hang in there...
-
-
14:40 - The pareto principle - 20% of your efforts produce 80% of your results.
This keeps us from being overly annoying. Reality is, eating out is terrible for you, so be picky.
-
15:15 - DUMP THE PROCESSED SEED OILS / VEGETABLE OILS!
Refined seed oils are huge contributors to inflammation and a lot of metabolic damage.[20-22] Request food be cooked in butter or olive oil if eating out (can mention allergies to soy and canola and such). Soybean oil, canola oil, and safflower oil are used everywhere -- chemically refined, never used prior to 50 years ago.
Trick: Go to McDonald's and get the beef patties only, they'll never be cooked in oil! But don't forget to enjoy yourself on occasions - remember the pareto principle.
-
18:00 - Note that age-related testosterone decline is not necessarily inevitable.
Great athletes can keep their testosterone levels high through age, well into their 60s.
-
20:00 - How do we "fight fire with fire"? Can supplements help? Not much...
There are a million test boosters using evidence-based ingredients. Take ashwagandha, for instance -- it can yield a 14.7% increase in testosterone.[23] "There's a difference between statistical significance and clinically-meaningful results". It's a reliable effect, but it's not a meaningful effect. Your amount of testosterone probably varies by that much on a daily basis. That's basically the same as getting 8 hours of sleep instead of 7.
-
22:00 - Going to need to go the pharmaceutical route
"So supplements, while they have their purpose, for testosterone improvement, there's no good evidence behind it. That's why, if you want to boost testosterone, you have to go the prescription pharmaceutical route."

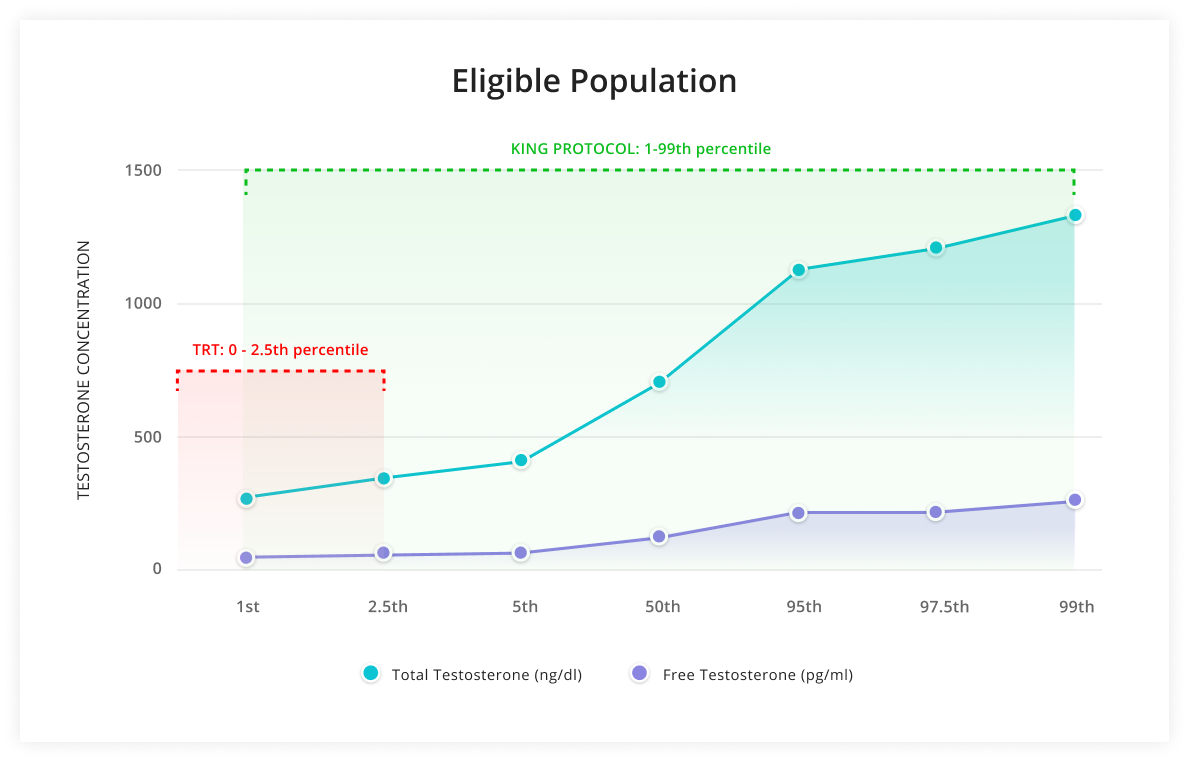
Unlike TRT, the Maximus KING Protocol can be used by a far greater subset of men, including healthy young ones.
-
23:05 - Testosterone replacement therapy (TRT) and its major issues
"The gold standard of treatment today has been testosterone replacement therapy, or TRT". TRT does work - you inject more to top off levels. But the problem is the way that it works -- exogenous testosterone tells your body that it doesn't need to produce more of its own, and the testicles essentially shut down and shrink. It promotes infertility. Paper: "Testosterone Is a Contraceptive and Should Not Be Used in Men Who Desire Fertility"[24] Any guys under 50, or those who want to maintain fertility should not be on TRT.
-
24:00 - Primary hypogonadism vs. secondary hypogonadism
Primary hypogonadism is when the testicles do not work - due to injury, disease, or genetic issue. If that's the case, then TRT is the first line of treatment. Reality: that's only a small percentage of guys - akin to type-1 diabetics.
Secondary hypogonadism is more akin to type-2 diabetes - it's environmental. The signal between brain and testes has been dampened for the major factors discussed above. Don't jump to injecting testosterone - that doesn't seem clinically correct.
-
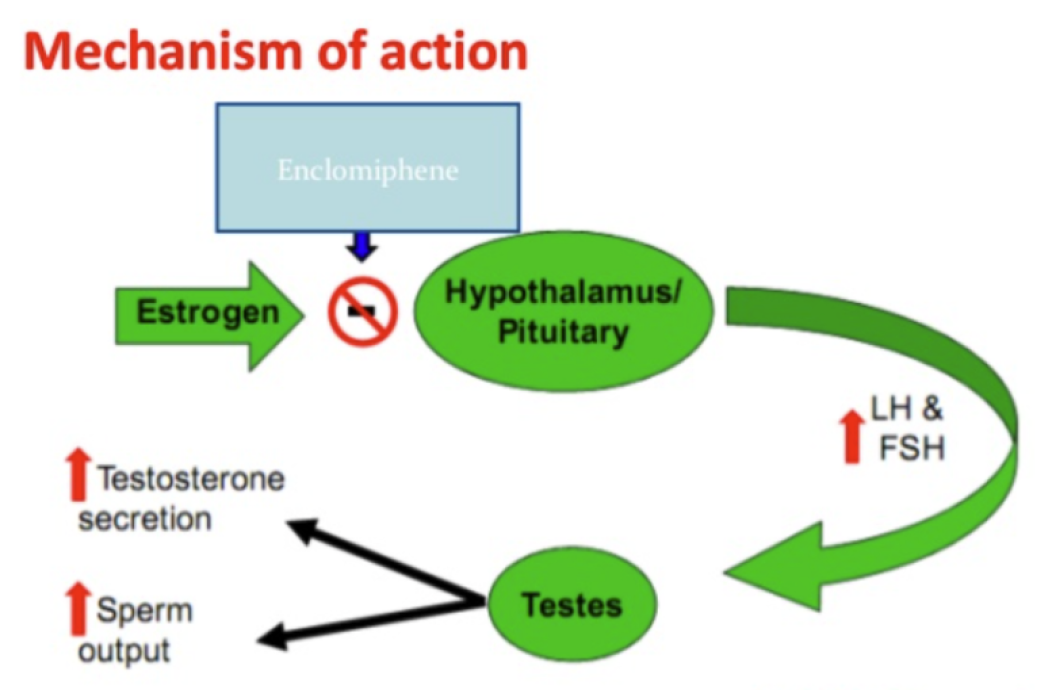
26:20 - SERMs - Selective Estrogen Receptor Modulators

A superior SERM: The Enclomiphene Mechanism of Action
SERMs started as anti-cancer drugs and are fertility drugs. SERMs selectively block the estrogen receptor - this causes the brain to want more, and to do that, it produces more testosterone by sending more LH (luteinizing hormone) and FSH (follicle stimulating hormone).
-
28:50 - TRT vs SERMs
On TRT, LH and FSH are completely shut down - can't produce their own testosterone or sperm. On SERM, LH and FSH are twice as high. Testicles grow with it if dosed high enough.
In addition, TRT is basically for life, and you have to run PCT to restart your own system if you want to get off of it. SERMs can be removed and testosterone just goes back down. SERMs have also been studied in healthy young men who don't want to risk fertility loss. Minimal side effects when using the right SERMs - no worse than placebo.
SERMs are far easier - just a pill. No creams or gels or injections with weird side effects (such as your gel rubbing off on a partner or kid).
-
32:00 - What's the gotcha? Why aren't SERMs more popular?

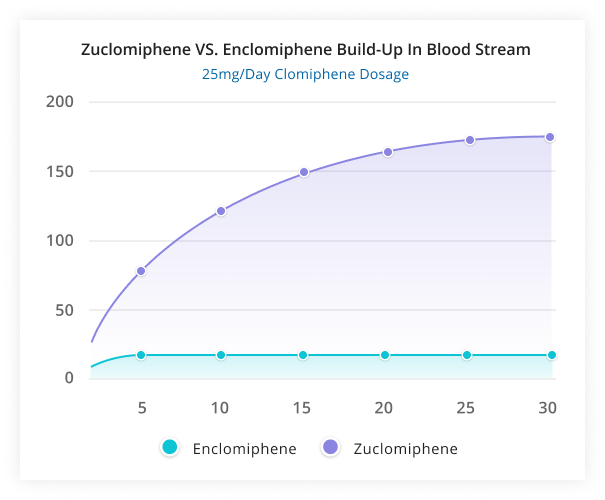
The problem with Clomid: The estrogenic zuclomiphene isomer lasts way too long. The solution? Remove it and use enclomiphene only!
The problem is that the most popular SERM is clomid, or clomiphene citrate, which is actually two drugs that are stereoisomers of each other. Inside is zuclomiphene and enclomiphene. Clomid is 62% enclomiphene and 38% zuclomiphene.[25-28]
Enclomiphene is most responsible for boosting testosterone, but zuclomiphene is an estrogen agonist - it mimics estrogen. While there's less zuclomiphene in clomid, the zuclomiphene has a very long half-life - weeks[29-31] compared to about 10.5 hours for enclomiphene.[25,29,30]
This leads to awful, estrogenic side effects over time in men.
-
33:30 - The problem with Clomid: Enclomiphene vs. zuclomiphene
So clomid causes a nice testosterone boost and feels great at first, but then zuclomiphene stays in the system for a long time, accumulating over time and wreaking havoc.
So within months, you're basically taking estrogen. Guys on clomid simply don't feel good after a while - they're more emotional, libido tanks, and they generally become more feminine.
-
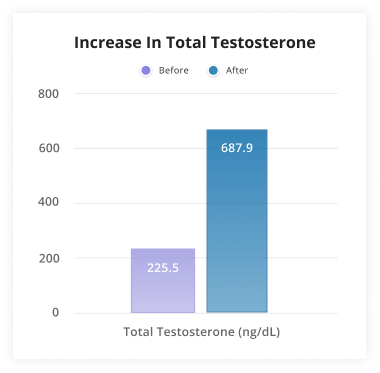
36:30 - The solution: Enclomiphene! Why not get rid of the isomer that's causing all the side effects?!

Enclomiphene and Total Testosterone
A pharmaceutical company did just that, ran trials on enclomiphene, and didn't see all of the clomid side effects.[25,26,32-38] It hasn't been available until recently, and now Maximus uses it.
Enclomiphene is the solution.
-
37:50 - Dr. Cam's personal experiences with both clomid and enclomiphene
Cam took Clomid 10 years ago, testosterone went from say 500 to 750, up 1.5x but with too many side effects -- not worth it. With enclomiphene, went from 450 to 900 - 2x gain, no side effects. This is consistent with the research.
-
39:00 - SERM mechanism and SERMs vs aromatase inhibitors
Be careful with aggressive aromatase inhibitors that block all estrogen, which is a bit too crude. Generally not taken standalone - estradiol gets cut in half and you don't want it too low either. SERMs are more selective. They increase testosterone and estradiol, but the estradiol won't bind because the estrogen receptors are blocked.
-
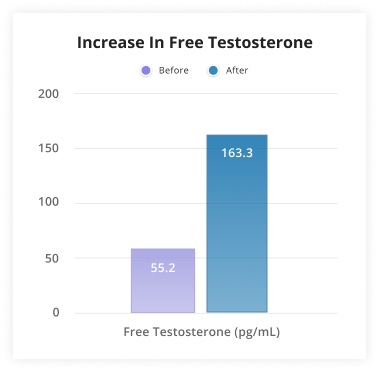
40:45 - Enclomiphene side effects?
Enclomiphene and Free Testosterone
Gynecomastia? Actually it's used to combat gyno.
Hair loss? SERMs also don't increase DHT levels proportional to testosterone -- DHT is the "aggressive hormone" that's blamed on hair loss. Dr. Cam notes that taking finasteride (a popular DHT blocker) is not good for sex drive, for some it's permanent loss.
DHT is important for competitiveness and virility - probably not a great idea to block systemically. Don't want it too low, don't want it too high either though. TRT causes high DHT levels in proportion[39-43] and enclomiphene keeps the proportion steady.[36]
Because of the research and its stable ratios, enclomiphene is much more "hair-safe" because it's not jacking up DHT levels disproportionately.
-
45:00 - Maximus uses 3rd party, at-home blood tests
Collects blood just before beginning medication - so that there's a clean baseline. "We treat symptoms, not numbers" - this is different from TRT. They retest after 30 days.
-
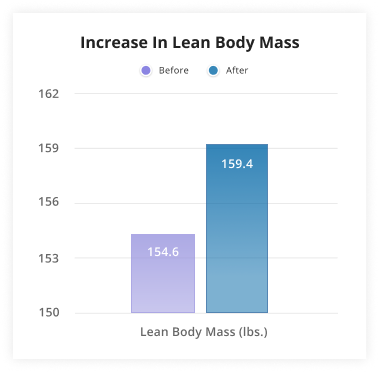
47:55 - Is this for getting huge and jacked?
Enclomiphene Lean Mass Gains
This is not better than testosterone for elite bodybuilders because it won't take you to supraphysiological levels. Your testosterone isn't going to 3000-5000 range like bodybuilders see.
The improvement range is usually 1.5x to 2x improvement.
-
49:00 - Will naturally high-T individuals get any benefits?
To answer Ben's question from 44:00 ("Can someone with already-high testosterone still double their levels?"), the answer is often the opposite of what many expect -- higher-T users get greater effects than those with low-T or those trying to recover from TRT. They'll go from ~200,300 to ~400,500.
The healthier you are to start with, the better your mind-body connection is, the better your testicles produce more testosterone. But it matters how you feel more than actual numbers.
-
50:00 - Testimonials
TFW "I now know what it feels to walk around like i'm the king."
CASE STUDY: 37 y/o male, 6'3, 250 lb, low T, was on TRT but wanted to stop.
After 2 mo on @MaximusTribe King Protocol, Total T increased 230 to 439 ng/dL, Free T increased 64.5 to 130 pg/mL!
2X ⬆️ T! Fantastic! pic.twitter.com/jATzTduZUp
— Dr. Cam Maximus ??????♂️?? (@DrCamMaximus) January 21, 2022
Testosterone Stimulation is so safe it's not just for guys with extremely low T!
This client is a fit professional whose Free T used to be in the 100s, but declined to 61 pg/mL in his 40s.
After 25 days on @MaximusTribe, Total T increased 2X, Free T increased 2.5X. Fantastic! pic.twitter.com/7sTHHNgNgF
— Dr. Cam Maximus ??????♂️?? (@DrCamMaximus) January 21, 2022
-
50:40 - Total Testosterone vs. Free Testosterone, and Reference Ranges
First, don't compare to average men - compare to healthy men. They don't look at age references as much as healthy references.
Free testosterone is not bound to proteins like albumin or SHBG (sex hormone binding globulin). The human body is intelligent and balances itself properly. But for some individuals, there's less free testosterone out there to bind to new sites. When SHBG is high, total testosterone goes high, but there's still not much free testosterone.

One way to increase free testosterone is with boron,[44] but we're not sure if that works in the long-term. Maximus advisor Dr. Eugene Shippen says that you shouldn't mess with SHBG - it's genetic, and you're used to what you have. So try to focus on free testosterone.
-
55:00 - Enclomiphene dosage for starters?
Since Maximus ships enclomiphene with the original blood test, it means they're providing the drug before knowing your scores -- so what dose do they start with?
The answer is 6.25 milligrams, which is the smallest dose generally tested in the research.[25,26,32-38] You don't need much - and can always go up (and in a few cases, down to 3.125 milligrams). Later on, Cam mentions that they have 8 different dosages they can prescribe.
While 12.5 milligrams was generally the best dose in research, that was in subjects with hypogonadism -- not the generally healthy Maximus Tribe member! In addition, starting conservatively is the best way to approach medicine. Dr. Cam is on 6.25 himself.
-
57:20 - Mike's testosterone levels... high total testosterone, but low free testosterone!
With a supplement, Mike got his total testosterone to go up from 681 to 791 (link to tests). However, free testosterone was only bumped from 63.5 to 66.1 - very low on the reference range! Didn't test for SHBG, but it's likely high.
-
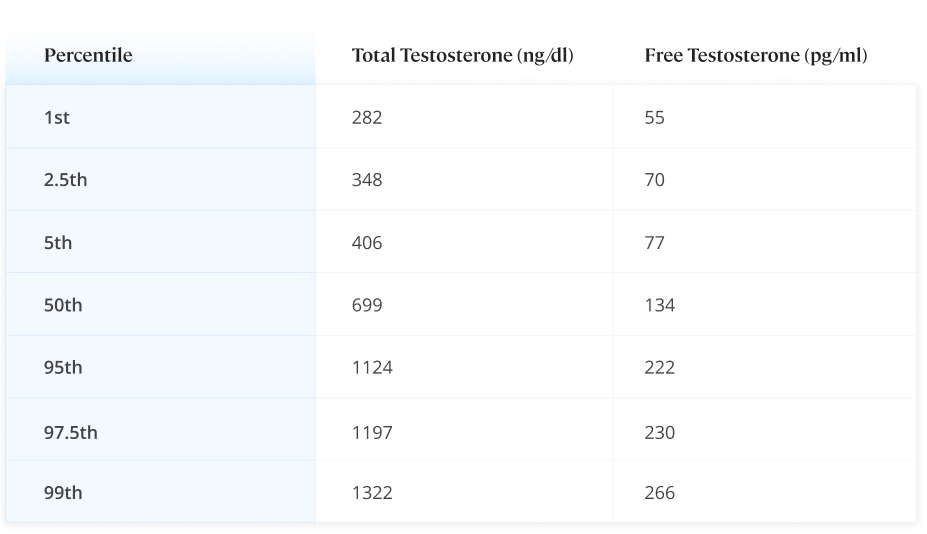
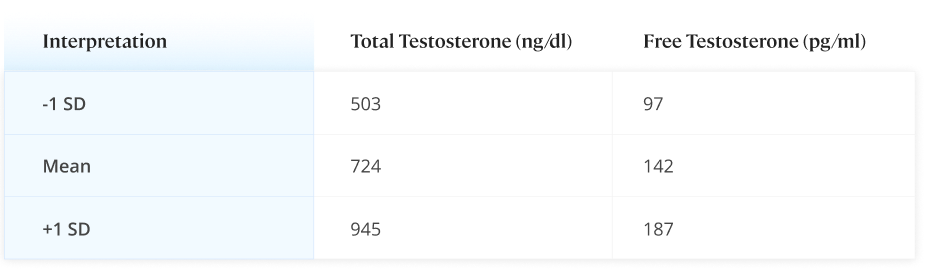
59:00 - Using better, more relevant reference ranges
To help with Mike's free testosterone levels, Cam references their preferred reference ranges with healthy 19-39 year old men, since the ones shown on blood tests are far too wide:

Maximus' Reference Ranges

Maximus' Testosterone Targets
Although above average on total testosterone, Mike is indeed multiple standard deviations away from the bell curve in terms of free testosterone.
-
1:00:00 - Muscle mass if improving free test?
Using clomid as a proxy study, 12 weeks of clomid use led to 5 pounds of lean muscle mass gains.[45] So it's possible Mike's situation would lead to some worthy gains.
-
1:01:00 - Ben's blood work - lower SHBG, lower total test, higher free test, easier muscle gains
This puts Ben at lower risk of diabetes, but he has more free testosterone and it's easier for him to put on muscle than Mike.
-
1:02:00 - Can TRT users transition to Maximus?
Ben shares some experiences where he was on "huge!" doses of clomid and felt awful, but it was the effort to get "back on line".
-
1:05:00 - At-home blood tests and the future of telemedicine
Dr. Cam explains the model and how it's going to change everything. From the comfort and convenience of your own home, paired with at-home tests, you can have a virtual clinic nearly anywhere, run additional blood tests if necessary, and make changes on the fly. This is the future - no more generic prescribing.
-
1:08:30 - Who do you talk to on the Maximus system?
There's always a board-certified licensed physician prescribing the medication.
-
1:09:10 - Adding in supplements and discussing vitamin D
Vitamins do have a purpose -- covering for deficiencies. For example, boron, Vitamin D, zinc, etc. If these are low, then you're in trouble no matter what.
In a validation trial in Los Angeles, 66% of their users came in with sub-optimal Vitamin D! We generally like 10,000IU a day - this will get the overwhelming majority of people into the proper range. Multivitamins generally have a pittance of vitamin D.

Don't forget your Hormone D
Vitamin D and other fat soluble vitamins are actually hormones! Dr. Cam references a paper that calls it Hormone D![46]
So make sure you don't have deficiencies, especially in the fat-soluble vitamins that are involved in testosterone production. This includes A,D,E, and K -- and Dr. Cam also adds in GG, for geranylgeraniol, which is part of a sidechain of Vitamin E that helps produce testosterone as well.
-
1:16:52 - The KING Protocol - "Self-improvement should not be done alone"
There are actually three parts to the Maximus program:
-
The lab tests, enclomiphene prescription, and vitamins

It's not just about drugs - it's about community and coaching too! See the Maximus KING Protocol
-
Doctor consults and health coaching
Eat, exercise, sleep, focus, and mindset coaching. Maximus preaches accountability.
-
The community
The company is called Maximus but the online community is called "Maximus Tribe". "Self-improvement should not be done alone" - having other guys your age pushing you, you're going to perform better. For instance, you can't do high-intensity interval training correctly.
So the users check in and track their streaks. They push each other in a positive way that guys enjoy. Ben mentions Tribe by Sebastian Junger.[47]
The Maximus community on discord is at discord.maximustribe.com - provided as a public service for free.
1:21:25 - We have a bigger mission out there - we're trying to promote a positive, healthy masculinity and make guys do better. If I double everyone's testosterone levels and they act like douchebags in the world, I haven't done any good to the world.
1:23:18 - Social is health. Loneliness is one of the best predictors of mortality.[48]
-
-
1:25:00 - Live coaching on Maximus YouTube
Radio show on Thursdays at 6:00pm PDT - Subscribe to the Maximus YouTube channel which is where it's hosted.
-
1:25:20 - Dr. Sepah teases his next supplement
It's magnesium acetyl taurate... stay tuned!
-
1:26:46 - Dopamine Fasting and Focus

Dr. Cameron Sepah pioneered Dopamine Fasting, a strategy both men and women should utilize!
We don't dig into it much this time, but the idea behind dopamine fasting is to take breaks from anything that gives dopamine hits (electronics, porn, shopping, emotional eating, gambling, etc) and focus on learning, relationships, creating, and health-promoting activities.[49] This is essentially a protocol to overcome the "addictiveness" of behavior addictions.
College students quitting Facebook in 2017 yielded 13 more hours per day and much more creative productivity.[50] "A man distracted is a man defeated"
-
1:28:25 - Future drugs coming - sexual enjoyment?!
Dr. Cam explains that he has a sexual enjoyment drug on the way that's more than just an ED drug -- it actually improves enjoyability and sexual intimacy.
Also there's a hair and beard growth drug that's not finasteride. This is a hormonal approach that can help with a thicker beard.
-
1:30:20 - Getting off enclomiphene?
The studies didn't do discontinuation protocols, but the clinical experiences have been positive in this light. Some users get off of it for travel reasons and then get back on. This is like adding fuel to the fire, but then take the fuel away, the fire stays.
Maximus offers a 90 day guarantee - if your levels don't go up, they'll refund you.
-
1:34:25 - "Testosterone is like destiny"
Exposure to intrauterine testosterone is very indicative of future status as testosterone. If your ring finger is longer than your pointer finger, then you've been exposed to a decent amount of testosterone.[51]
"The amount of testosterone you're exposed to in the womb, which shows up in how long your fingers are, basically predict your athletic performance... It actually made me sad -- because no matter how hard you tried, how hard you train, it's almost predestined. You won the genetic lottery in terms of your testosterone and if you didn't, guess what - you get last place in the race and that's the card that you're dealt with.
But literally for the first time in history, you have the ability to take control of your destiny. If you're on the lower end of the testosterone spectrum, you don't have to be anymore. You can literally go from being a low performer to a high performer."
-- Dr. Cameron Sepah on the PricePlow Podcast
- @DrCamMaximus (Twitter, Instagram) Note: many of Cam's legendary Twitter threads are on his old Twitter account, @DrCamRX
- https://www.maximustribe.com
- http://discord.maximustribe.com
- The Maximus Podcast


Watch the Maximus Introduction:
![]()

Comments and Discussion (Powered by the PricePlow Forum)