Regular readers of this blog will recognize Dr. Cameron Sepah as a previous guest on one of our most popular podcast episodes. He is the founder of Maximus Tribe, a company whose mission is to provide ambitious, high-achieving men with authentic community and appropriate medical support to help them realize their full potential.
PT-141 (Bremelanotide) is a melanocortin agonist that boosts libido - but it's even more synergistic with tadalafil (Cialis). Learn how this is the next generation ED drug combo in this article, courtesy Maximus Tribe and their Lover Protocol
To that end, Dr. Sepah and his team of physicians have developed two pharmaceutical protocols designed to help men get the absolute most they can out of life.
First was the King Protocol, which uses enclomiphene to raise testosterone levels in men with hypogonadism. In PricePlow Podcast Episode #062, we talked with Dr. Sepah all about the King Protocol: specifically, the drawbacks of traditional testosterone replacement therapy (TRT) and why optimizing male hormones through the use of enclomiphene is a better strategy.
Announcing the Maximus Lover Protocol
Today we're excited to announce that Dr. Sepah is back again – and this time we'll be talking about the Maximus Lover Protocol, a combination of erection-boosting tadalafil (Cialis) and a scientifically validated aphrodisiac drug called PT-141 (bremelanotide), which we'll get into below. This protocol is designed to improve men's sexual lives by synergistically targeting different mechanisms involved in libido and arousal.
Learn the background on the PricePlow Podcast Episode #070
We had Dr. Cam back on the podcast to explain the protocol with his own words, and you can listen on Episode #070 of the PricePlow Podcast. The video is linked here on YouTube, but we can't embed it due to the adult nature of the content.
Below, we provide greater research on the research behind these two ingredients, which have been shown to synergize incredibly well for improved erectile function and pleasure. We'll show a couple exciting clips from the podcast, and then start with the background:
Low Libido and Erectile Dysfunction: A Concern For Men Of All Ages
We've all heard about, and perhaps experienced first hand, the decline in sexual function that afflicts most people as they age. We tend to think of this problem as afflicting only the middle-aged and the very old, but in reality, loss of libido and arousal can affect the relatively young.
In fact, by the time a man turns 40 years old, the probability that he's experienced some degree of erectile dysfunction is about 40%! Each successive decade of life increases his probability of ED by an additional 10%.[1] And, as we learned from Dr. Sepah in the podcast linked above, a staggering amount of men in their 20s use ED drugs for various reasons.
The situation is much the same with hypogonadism (low testosterone) – although we think of it as a problem affecting the very old, the reality is that hypogonadism is probably under-reported. According to one estimate, 40% of men over the age of 45 have clinically low testosterone levels.[2]
Unfortunately, hypogonadism is affecting more and more young men each year. For an in-depth discussion on why this is the case and what you can do about it, check out our article from March of this year on the Maximus Tribe King Protocol, Is Enclomiphene the Testosterone-Enhancing Drug We've Been Looking For?
The wide and increasing prevalence of hypogonadism is a problem because not only can hypogonadism cause ED, but it can also cause lack of sexual desire or low libido.[3]
Erectile dysfunction and lack of sexual desire are not the same
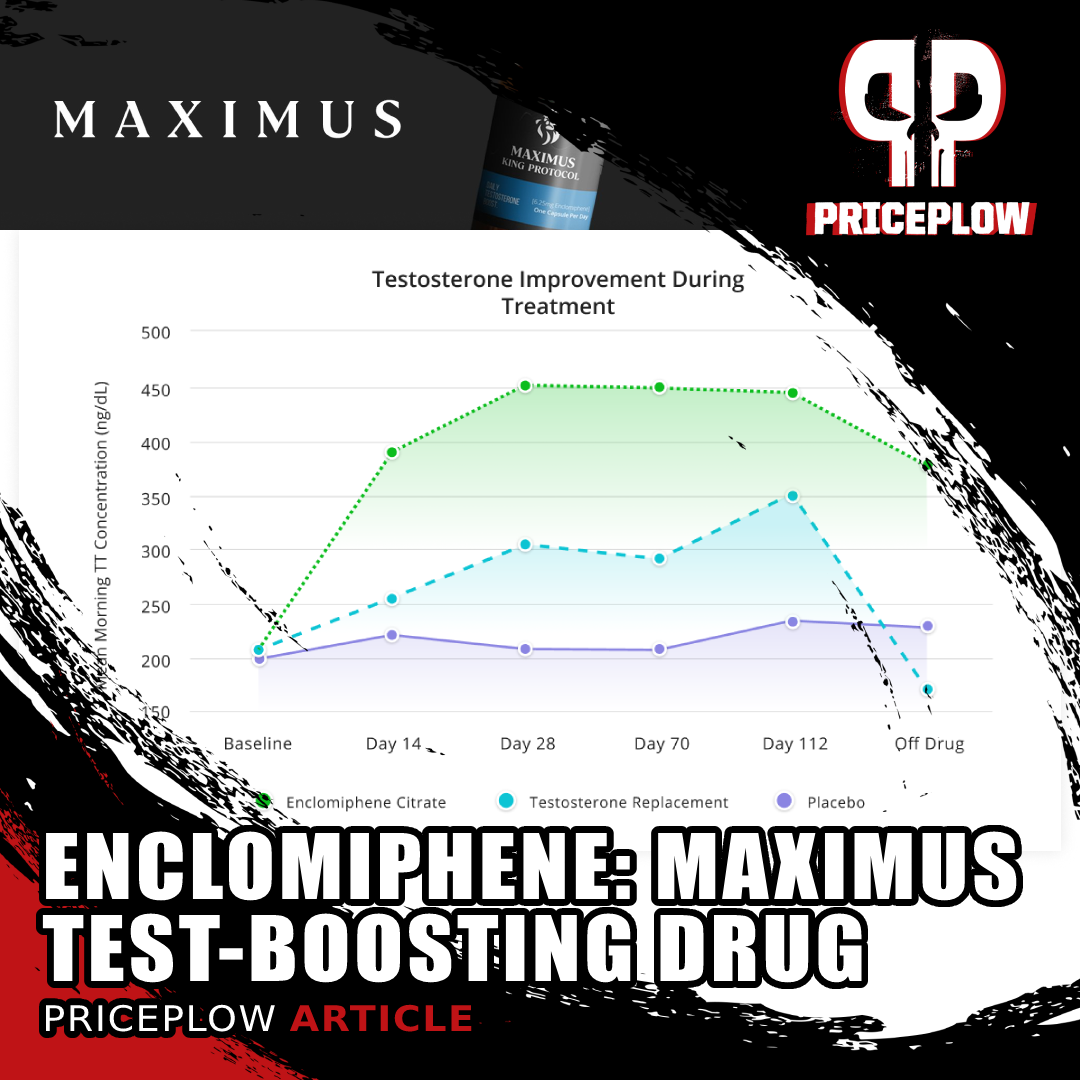
Enclomiphene: The Maximus Test-Boosting Drug that is a better alternative to TRT
You probably noticed that the groups of men with ED and low T are roughly the same size, and there's probably a lot of overlap between them, but we should still bear in mind that erectile dysfunction and lack of sexual desire are not necessarily the same thing. Being unable to perform when you want to is one thing – not wanting sex is another problem entirely, one that is far less frequently discussed or addressed than failing to get an erection.
If you have low libido, just taking Cialis probably isn't going to improve your sex life that much, because Cialis doesn't increase sexual desire – it improves your body's capacity for responding to sexual desire.
Don't just take our word for it though – Eli Lilly, the manufacturer of Cialis, explicitly states that "Cialis (tadalafil) does not increase a man's sexual desire, sex drive, or libido."[4]
Ideally, you want to treat both dimensions of sexual dysfunction: desire and ability to perform.
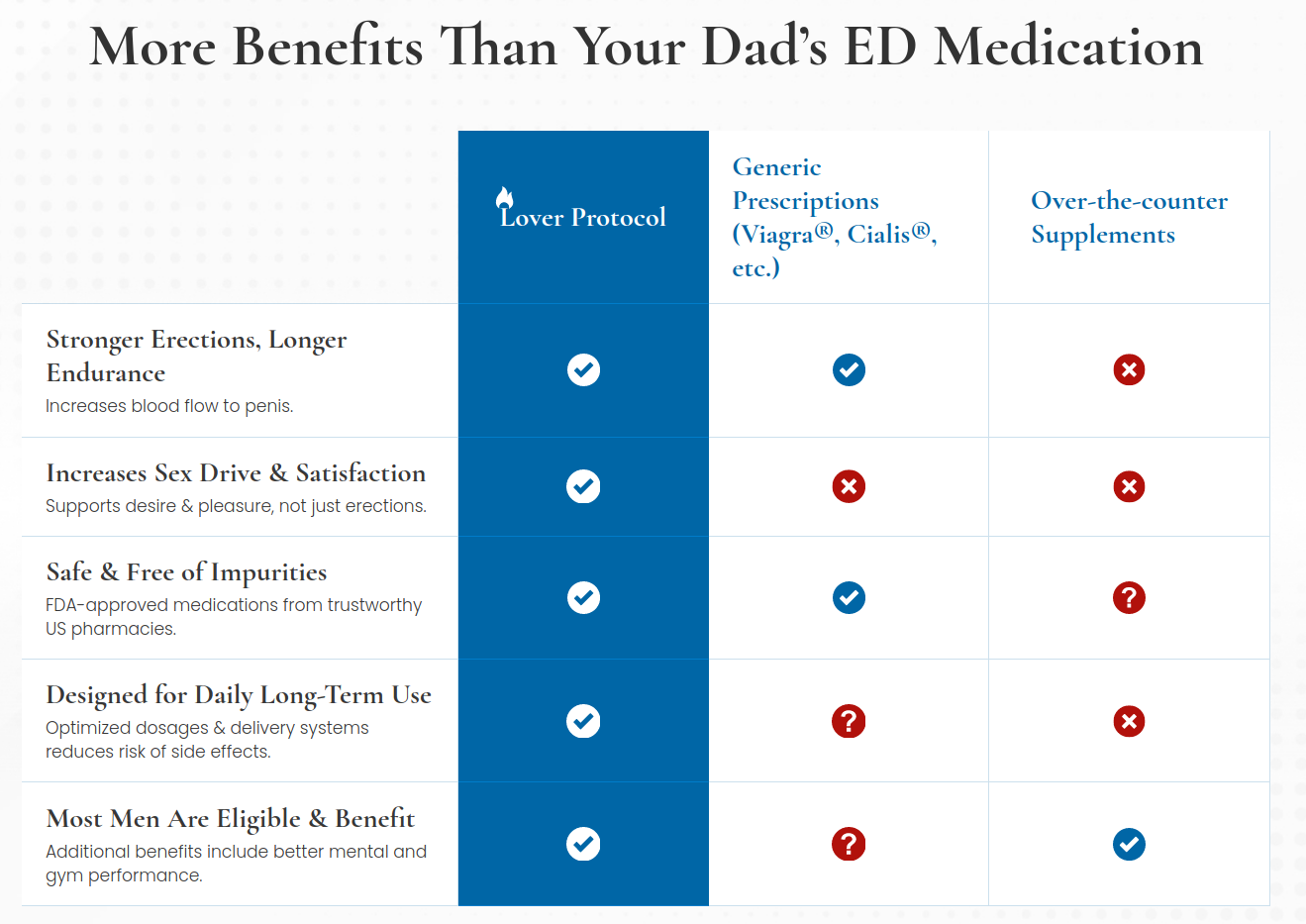
The Maximus Lover Protocol Treats Both Sides of Sexual Dysfunction
Dr. Sepah and his team had this in mind when they formulated the Maximus Lover Protocol. That's why this Protocol combines tadalafil with a drug called PT-141, or bremelanotide. As we'll see, not only do these two drugs complement each other, they also synergize: Certain effects of these drugs in combination have been shown to surpass what each drug can achieve on its own.
-
Tadalafil (brand name Cialis): mechanism of action
Cialis, also known as tadalafil, belongs to the same category of drugs as its famous cousin, Viagra. These drugs inhibit an enzyme called cyclic guanosine monophosphate-specific phosphodiesterase type 5, abbreviated to PDE5. We call these drugs PDE Inhibitors.[5]

Phosphodiesterase-5 inactives cGMP, a messenger molecule that mediates the vasodilatory effects of nitric oxide (NO). Inhibiting PDE5 potentiates the effects of NO.[6]
PDE5 is responsible for converting cyclic guanosine monophosphate (cGMP) to 5'-GMP.[5]
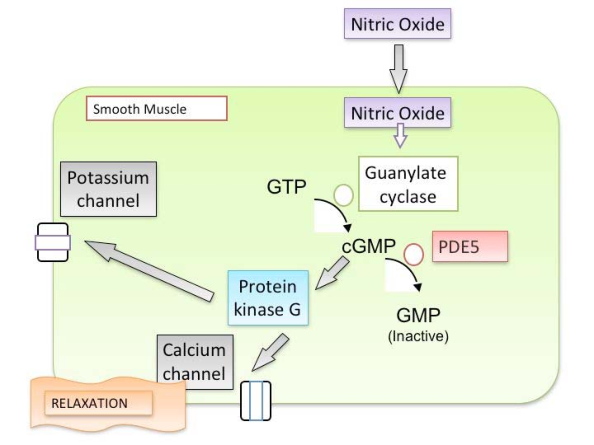
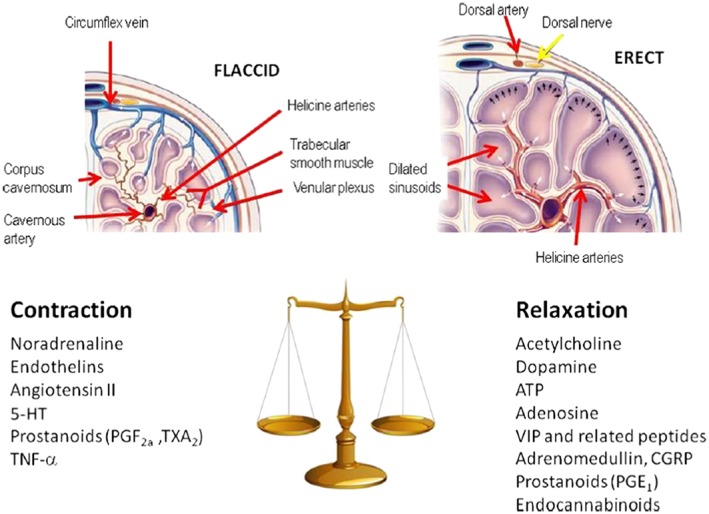
Inhibiting PDE5 raises your intracellular levels of cGMP, which matters because cGMP activates another enzyme called protein kinase G. This effect ultimately decreases intracellular calcium in smooth muscle, causing a relaxing effect in smooth muscle tissue.[7] This leads to benefits in terms of blood pressure, reduced lower urinary tract symptoms caused by BPH (benign prostatic hyperplasia, or "enlarged prostate"),[6] and erectile dysfunction (ED).
Ultimately, the relaxation of smooth muscle tissue allows for penile engorgement,[8] as the interior of your penis is lined with smooth muscle cells.
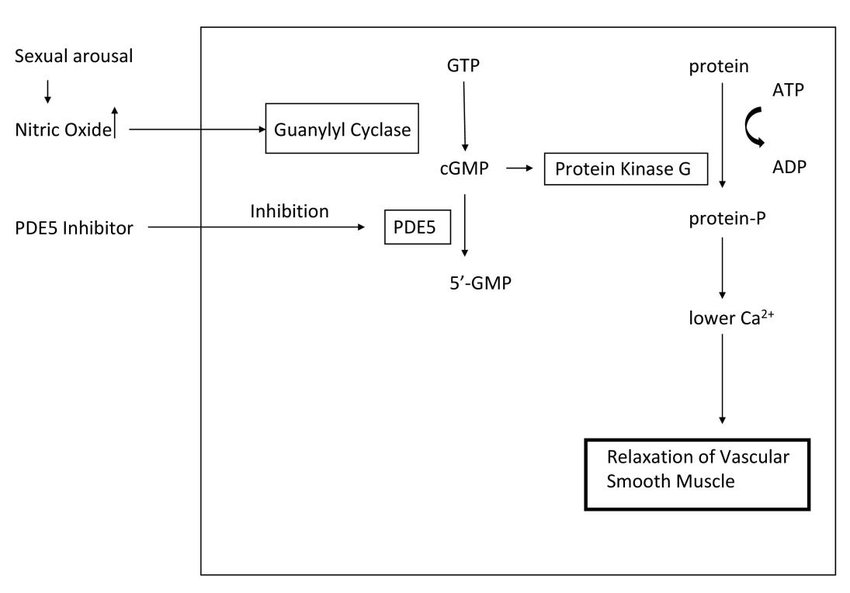
However, smooth muscle relaxation does not automatically lead to erections: as you can see from the diagram below, sexual arousal mediated by neurons is also necessary for increased nitric oxide secretion to cause penile engorgement.

Cialis (tadalafil) inhibits PDE5, the enzyme that degrades cGMP to 5'-GMP, effectively increasing cGMP levels and amplifying the erectile response to nitric oxide.[7]
Tadalafil (Cialis) vs. Viagra (sildenafil)
Most readers have probably realized at this point that tadalafil has the exact same mechanism of action as sildenafil (Viagra), a drug with which most men have at least a passing familiarity. So what makes them different?

Mechanisms of Penile Erection[5]
The main difference is that tadalafil has a longer half-life than sildenafil – 17.5 hours vs. ~4 hours.[9] Another lies in the fact that tadalafil's absorption, unlike sildenafil's absorption, is not affected by food.[10] This means that the patient can take Cialis/tadalafil whenever he wishes.
These two key properties of tadalafil make it a much more user-friendly drug, allowing men to initiate sexual encounters with their partners more spontaneously when taking it than they would on Viagra/sildenafil. Largely for this reason, patients and their sexual partners prefer Cialis over Viagra by a wide margin: a survey of 100 heterosexual couples in which the male had clinically diagnosed ED found that 79.2% of the women surveyed preferred that their man take Cialis. Only 15.6% of those women expressed a preference for Viagra.[11]
There is also the fact that long-term tadalafil administration has been shown to raise the all-important testosterone-to-estradiol (E2, a type of estrogen) ratio.[12] A similar effect has not been observed for sildenafil.
The athletic benefits of tadalafil
Although tadalafil has long been rumored to directly increase athletic performance, peer reviewed evidence to support this proposition is lacking.[13]
However – tadalafil may improve the body's response to exercise. One randomized, double-blind, placebo-controlled study found that men who took Cialis had higher levels of testosterone and cortisol following exercise, while men who took the placebo only had higher levels of cortisol.[14]

Dr. Cameron Sepah is back on the PricePlow Podcast to introduce The Maximus Lover Protocol
Let's unpack that a bit. Cialis caused the men to secrete testosterone in response to exercise – and it also increased the amount of cortisol they secreted. Now, higher levels of cortisol following exercise might sound like a bad thing, given cortisol's reputation as a catabolic stress hormone. But in fact, spikes in cortisol caused by exercise are usually a good thing, and help your body adapt to the exercise stimulus (i.e. become fitter).[15]
Another study found that in non-obese men with mild ED, tadalafil administration increased abdominal lean mass (muscle), probably because of its effects on insulin secretion, estradiol (E2, estrogen) levels, and endothelial function.[16]
Based on its ability to increase muscle mass through these key mechanisms, we strongly believe that there's a high probability that tadalafil increases the anabolic response to exercise, although we are not aware of any study that examined this specifically.
PDE Inhibitors Can Reduce Blood Pressure In Pulmonary Hypertension
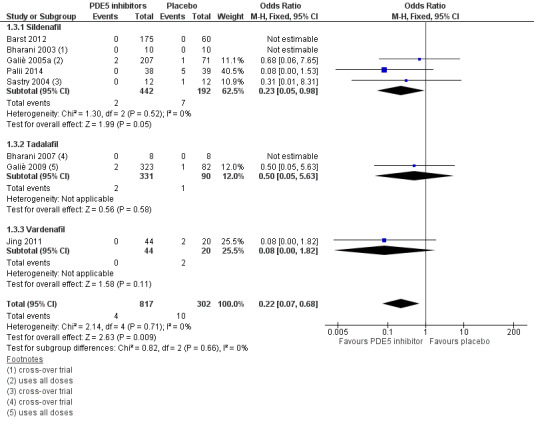
In order to evaluate the hypothesis that PDE5 inhibitors might improve whole-body cardiovascular function through their relaxing effect on smooth muscle, a large 2019 meta-analysis looked at over 36 studies with a cumulative total of 2,999 participants.[17]

A meta-analysis shows that PDE5 inhibitors reduce overall mortality![17]
The authors of this meta-analysis found that there's clear evidence PDE5 inhibitors have clinical benefit in a specific type of hypertension called pulmonary arterial hypertension (PAH).[17] They also found that PDE5 inhibitors may benefit patients with other types of hypertension, although the evidence is less clear.
Unfortunately, the data reviewed in this meta-analysis indicated that PDE5 inhibitors may cause harm in cases of valvular heart disease[17] – so if you have this condition, talk to your doctor about whether you should take tadalafil/Cialis.
Why not just take tadalafil on its own?
The main answer to this question is that, as we briefly touched on above, PDE5 inhibitors do not increase sexual desire. They make it easier to get an erection in response to arousal, but they do not cause arousal.
Many men do not respond to PDE5 inhibitors – this seems to be predicted by hypogonadism, for which, remember, Maximus has developed the enclomiphene-based King Protocol.
But as it turns out, there is a drug that can increase sexual desire and improve outcomes in men who don't respond to PDE5 inhibitors.
That drug is PT-141, also known as bremelanotide:
-
PT-141 (Bremelanotide) – Synergistic with PDE5 inhibitors

Bremelanotide is also known as PT-141, and was originally prescribed for women as Vyleesi
PT-141 is a drug also known as bremelanotide that has been shown to act directly on the cluster of neurons responsible for initiating sexual arousal. It's available as an injectible prescription drug named Vyleesi for premenopausal women suffering from "hypoactive sexual desire disorder",[18] but it's not just for women, and doesn't necessarily need to be injected.
Before getting into the data, it's worth listening to Dr. Sepah discuss the background of this drug's discovery, which you can hear around the 44:30 marker of PricePlow Podcast episode #070. Researchers had been looking at melanocortin agonists (melanotan-1 and melanotan-2) for other reasons -- sunless tanning[19,20] -- but they also found that the melanocortin receptors targeted by these drugs were also responsible for sexual function.[21] This then led to research on these "melanocortins" for the treatment of both male and female sexual dysfunction.[22]
While melanotan-1 and melanotan-2 didn't pan out as tanning agents nor sexual enhancement drugs, it led researchers down a path towards better melanocortin agonists that could specifically target sexual function. This eventually led to PT-141, which has been researched heavily for the past couple of decades.
PT-141 / bremelanotide research

The Maximus Lover Protocol Benefits - Image courtesy Maximus
In one study that was conducted on both rats and humans, researchers found that rats who had received PT-141 had much higher neural activity in the paraventricular nucleus (PVN), a neural structure located in the hypothalamus region of the brain that plays a huge role in sexual stimulation.[23]
In the 24 human patients who took PT-141 as part of this study, the drug increased erectile activity by a factor of 3, meaning that the PT-141 group got erections three times as often as the placebo group.[23]
Goes where ED drugs don't, and often works when they don't...
Because it has a different mechanism of action, PT-141 has been shown more than once to improve sexual function in men who did not respond to a PDE5 inhibitor (usually these studies are done with Viagra/sildenafil, but the results apply to Cialis/tadalafil as well).[24,25]
...but the combination with PDE5 inhibitors is where the real success is at

PT-141 works even better in combination with a PDE5 inhibitor![26]
More importantly, the combination of a PDE5 inhibitor with PT-141 works better than the PDE5 inhibitor alone, even in men who do respond to PDE5 inhibitors.[26]
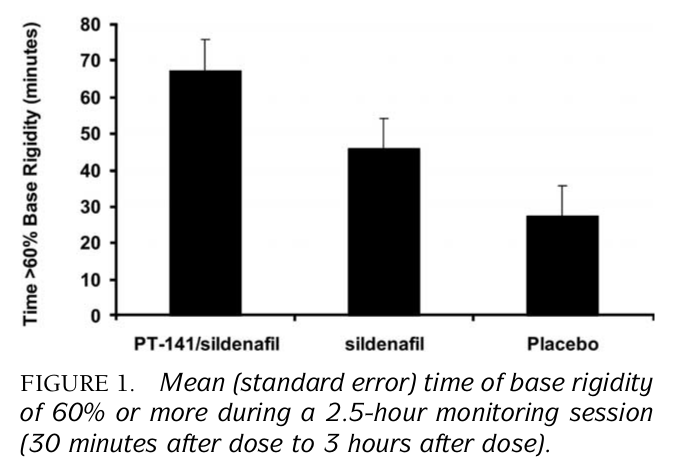
In one 2005 double-blind, randomized, placebo-controlled study, male subjects were given sildenafil, a placebo, or the combination of sildenafil and PT-141. They were then shown a 30 minute erotic film, after which their erectile activity was monitored for the next 150 minutes. No mention of orgasm or ejaculation is in the study, but from what we can tell, they were likely advised not to achieve climax within the 150 minutes.[26]
The results were profound: The men who received sildenafil and PT-141 were erect for nearly 70 minutes of this 150 minute period – compare that to men who received only sildenafil (45 minutes) or the placebo (25 minutes).[26]
This study is a major basis for the Lover Protocol - these two drug classes combined is where the greatest number of users may see incredible sexual success.

Conclusion: The Lover Protocol Includes Both
Of course, tadalafil and PT-141 may have unwanted side effects in a number of cases. These are almost always mild, and non-threatening. With the low dose used in the Maximus Lover Protocol, and a non-injected, sublingual tablet, it should not be strong. Dr. Sepah is very wise to go for the minimum effective dose of all drugs they use - never too much.
It's not just about drugs - it's about community and coaching too!
Remember, tadalafil and PT-141 are prescription drugs, so do not take them without first consulting a physician and obtaining a legitimate prescription.
Fortunately, if you're interested in seeing whether you medically qualify for The Lover Protocol, Dr. Sepah and the rest of the Maximus physician team can review your case in a remote video appointment that can be scheduled at MaximusTribe.com/lover.
Overall, the Lover Protocol represents a substantial innovation in the treatment of erectile dysfunction and lack of male sexual desire.
As mentioned in both of our Dr. Cam podcasts linked throughout this article, we always focus on metabolic health first. But while you're doing everything you can to clean up your diet, sleep, and overall lifestyle, these protocols can help push you over the top to greater masculine success.

Comments and Discussion (Powered by the PricePlow Forum)