The last few years have served as the Renaissance of supplement dosing. Products that lived and died by “Svelt Swole” proprietary blends have fallen to newcomers that promise consumers “fully transparent” labels that list every ingredient down to the nanogram. The 2010s are a golden era of consumer awareness — as we now know how much stimulant we’re getting per scoop and can titrate our products to match our individual tolerance.
The caffeine dosage arms race
This awareness has also cursed the thinking lifter (hint: all of us living in PricePlow Nation) with a newfound curiosity for how far we can push these dosages. The desire to one-up their competition forces companies to meet our expectations with ever-heavier serving sizes. This heavy-handed serving size trend is most noticeable with our beloved stimulant, caffeine. Not too many years ago, “spicy” products contained ~250mg of caffeine per scoop. A typical energy drink contained 110mg of caffeine per can. We now live in an era where the average pre-workout contains 300mg of caffeine. There are now consumer energy drinks that deliver 300mg of caffeine per can.
So why are we here? Our society's addiction issues aside, we’re interested in another angle to caffeine dosing: performance.
Today, we will dive into just how much caffeine is tolerable for the average athlete, how much we can hang with our best xanthine friend, and if there’s any level of performance benefit to higher doses once you’ve worked your tolerance up to them. If you’re ready for the insane gains (yet potential bowel movements) that come with exploring uncharted xanthine-stimulant territory, let’s get to the science.
The Basics: Safety and Background for Industry Shift
There is no defined “safe” universal caffeine dosage. Some people can down 16oz of caffeine feeling nothing while others drink one cup and shift into “the world is ending”-tier anxiety. Truly, there is an endless list of health conditions that may force an individual to avoid caffeine.
To explore athletic safety, we will use a “healthy adult” model. The keen-eyed amongst our readers may point out that there is no “healthy” ideal — which is true. We would like you to think of our “healthy ideal” as an adult without major chronic health conditions. We will not comment on the status of caffeine doses in children and teenagers, as much of the current conservation is confounded by little research and postulation.

Another "extreme" label, Metabolic Nutrition's E.S.P. Extreme touts 750mg caffeine on the front of the tub... but that's only if you take an insane three scoops! Should it be marketed that way?
The European Food Safety Agency (EFSA), Health Canada, and the US National Academies of Science agree that ~400mg/day does not raise major health concerns.[1-3] This mutuality amongst governing bodies infers that 400mg of caffeine may be our recommended limit for those wanting to adhere to the findings of modern medicine. For those hardcore stimulant freaks that want to push the envelope, you can assume that ~400mg of caffeine is a good total daily driver to work your pre-workout dosing around.
This finding may explain the industry shift towards “heavy-scooped” stimulant dosing. If the upper limit of caffeine is 400mg, lifters likely found this out through n=1 gym sessions. For those too young to remember, it was once common place to triple-scoop consumer pre-workouts. It is reasonable to assume that companies discovered this practice through social media and titrated doses up to appeal to the more “hardcore” consumer.
Pregnant Women
Interestingly, the paradigm that pregnant women should not use any caffeine may be a distant memory within the next few years. The EFSA believes the safe upper limit of caffeine per day in a pregnant woman may be between 200 to 300mg of caffeine. Medical authorities in other countries agree.[1,4-5] You may notice this is close to our “I care about my health” caffeine limit. As this research is still developing, it is likely prudent for pregnant women to stick to a lower caffeine intake.
A striking comment from a recent paper by Edmund et. al on the impacts of caffeine on pregnancy is the following:
“Early miscarriage is certainly more common in women who drink substantial amounts of coffee in early pregnancy.[7] However, we do not know whether continuing high consumption puts the fetus at risk, or whether sustained consumption is simply a marker for a pregnancy that is already doomed, because an increased aversion to coffee is, along with nausea and vomiting, a consistent early feature of a healthy pregnancy.”[8]
Long story short: if you’re pregnant, stick to the safe side with zero or ultra-low caffeine doses while the experts battle this out.
Did I Take Too Much? Side Effects of High Doses
Assume you consumed a ton of caffeine and then stumble into this article. A sense of dread may overcome you if you went over the doses we mentioned. Thankfully, there are telltale signs that let clinicians know if an individual’s systemic caffeine concentration is over the “harm” threshold. People that overdose on caffeine typically experience dizziness, diarrhea, enhanced thirst, insomnia (unsurprisingly), headache, fever, and irritability.[10,11] If someone presents to an ER with these symptoms and describes a classic story of “I didn’t know you had to dilute cold brew coffee” - it’s easy to tell that caffeine overdose has occurred.
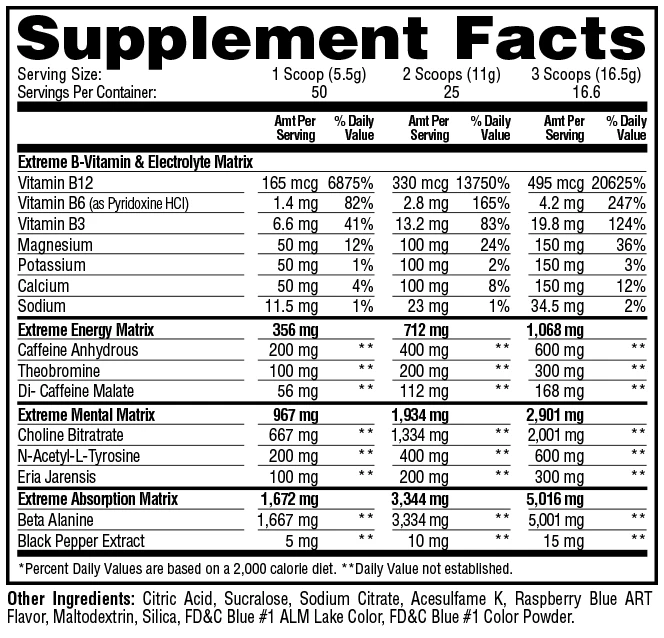
This label of the above product ignited a firestorm on social media. Note that there's two forms of caffeine, yielding ~250mg total per scoop. Is there a benefit to 750mg total, and if so, how big and tolerant would you need to be?!
More serious side effects include dyspnea, vomiting, metabolic acidosis, hallucinations, confusion, angina, arrhythmias, palpitations, and convulsions.[10,11] Caffeine appears to cause lethality through decreased blood flow to the heart. Reduced blood flow to the heart is a variable defined clinically as “reduced venous return”, which may cause shock.
Caffeine causes this massive array of side effects due to the amount of receptors it interacts with. The interaction of caffeine with adenosine 1 receptors (A1) are likely responsible for the neurologic symptoms. Caffeine can also inhibit phosphodiesterase, leading to increased cAMP and calcium within cells. It can even trigger the release of catecholamines, causing side effects that resemble disorders of sympathetic nervous system overstimulation.[12]
Caffeine-induced death appears largely in case studies. While toxicity is common, deaths due to caffeine alone are rare.[10-11] However, it is likely that many of the caffeine-related fatalities are caused by underlying issues exacerbated by the caffeine bolus causing the overdose. So if you’re wondering if recent products encouraging consumers to take 700mg of caffeine at a time are really dumb... yes.
Caffeine and Blood Pressure
Caffeine is a polarizing compound in vascular research. Some trials have attached caffeine intake to increases in risk of cardiovascular disease while others describe no effect.[28] Some even show that caffeine may reduce the risk of cardiovascular disease.[29] The disagreement stems from caffeine dipping its paws into many vascular processes.
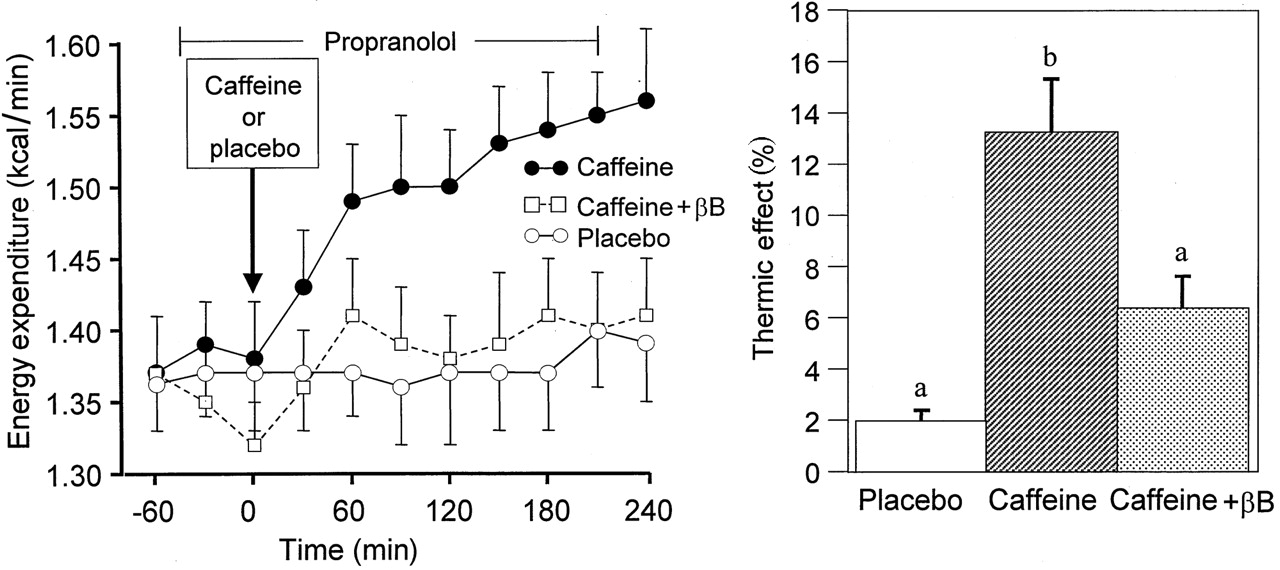
Caffeine increases energy expenditure by roughly an extra 0.15 calories per minute. Not huge, but we'll take it! But what happens when the dose gets absurd?
Caffeine, as noted, antagonizes adenosine receptors. However, xanthines also inhibit phosphodiesterase, reduce the amount of calcium available to vascular smooth muscle, and appears to influence levels of cAMP through receptor modulation. Below, we will cover the direct impact of caffeine on the vasculature.
The nitric oxide connection
Caffeine may stimulate endothelial cells to release nitric oxide.[30] Caffeine activates nitric oxide synthase (NOS) by increasing the amount of intracellular calcium - so we have to talk about molecular biology for a second. To maintain optimal cellular function, calcium is sequestered intracellularly into an organelle that allows for a steady on-demand release -- which we call the endoplasmic reticulum. Calcium is released from the endoplasmic reticulum through ryanodine receptors. These receptors require a base level (threshold) of calcium present in the cell to activate -- a process called calcium-induced calcium release.[31] Caffeine may reduce the threshold of calmodulin activation, allowing the intracellular levels of calcium to raise.[30]
NOS requires the protein calmodulin to work -- which only binds to NOS in the presence of calcium.[31] Thanks to caffeine, calmodulin and calcium can form a complex.[30] The calcium-calmodulin complex favors NOS activation -- leading to nitric oxide production from oxygen and L-arginine. The nitric oxide formed diffuses out of the cell to influence nearby cells to increase their levels of calcium and nitric oxide production. [30,31] Nitric oxide is a potent vasodilator and may allow for increased blood flow to tissue impacted by caffeine.
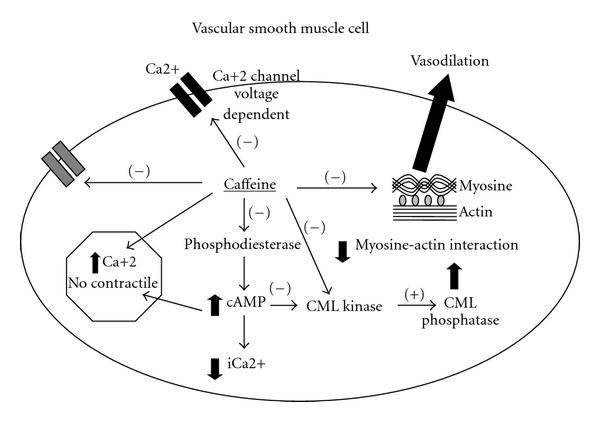
The Caffeine-Calcium Connection: "Vasodilation produced by the direct effects of caffeine on the VSMC. Caffeine inhibits the voltage-dependent Ca2+ channels and the entrance of calcium to the cytoplasm. In addition, it inhibits the IP3 receptor and increases the “non-contractile Ca2+. Due to its antiphosphodiesterase action, there is an accumulation of cAMP, which increases the non-contractile Ca2+, diminishes cytoplasmic Ca2+ (iCa2+), and inhibits Myosin Light Chain Kinase (MLC Kinase). Therefore MLC phosphatase predominates and there is vasodilation. Caffeine also directly inhibits MLC Kinase and the actin-myosin interaction."[30]
This mechanism also occurs within vascular smooth muscle -- leads to muscle contraction. While this smooth muscle contraction would lead to vasoconstriction, the impact of caffeine on phosphodiesterase leads to an increase in cAMP.[30] This increase in cAMP inhibits contraction processes within the smooth muscle cell. The net effect in vascular muscle still appears to be vasodilation due to this cAMP bump.[30]
However, those with preexisting hypertension may experience transient increases in blood pressure. Caffeine appears to increase blood pressure in those experiencing hypertension and other metabolic issues.[32] This may be because of “stiffer” blood vessel created by arteriolosclerosis— but this is postulation.[33] Those at risk of hypertension or atherosclerosis may want to defer to healthcare professionals before using high doses of caffeine.
How Much Caffeine is Helpful?
We now arrive to the fun part of this guide. It turns out that many groups share our curiosity. As most of our audience are weight-room vikings, we’ll start with specific research covering strength-sports performance. A review featuring the king of natural bodybuilding research, Eric Helms, settles at a recommended dose of 5-6mg/kg of bodyweight. If we take an individual that weighs roughly 185lb, this puts their optimal dose range between 415mg-498mg of caffeine — which is nearly in line with what we concluded earlier.[13] A review that focused on caffeine specifically arrives at a similar conclusion — doses around 5-6mg/kg per day were better than lower doses.[14]
~400mg caffeine is the dose that will get most people closest to 5-6mg/kg per day, where several research studies have proven successful. But can going higher for the big guys (who are a 'healthy' big, not obese) be even better?!
There are some investigations that demonstrated 7mg/kg as being safe. However, one trial showed that 7mg/kg did not significantly improve performance above a dose of 6mg/kg in cyclists.[15] When we attempt to search for doses of 8mg/kg or higher... most research search queries cover caffeine overdose so it is perhaps prudent to stick to a dose of 5-6mg/kg per workout. We found one study that explored the benefits of 13mg/kg — however, the investigators concluded that caffeine hits a point of diminishing returns past 6mg/kg [27]
Caveats
As with anything, there are caveats to the 5-6mg/kg “gold standard” of caffeine dosing. Mixed xanthines, barring theacrine, are subject to massive tolerance development with repeated dosing. The answer to tolerance should likely not be upping the dose as the harmful side effects of caffeine, like high blood pressure, may not dissipate with long term use.[16] Another massive caveat is how an individual metabolizes caffeine. Those that possess a CYP1A2-C genotype experience a reduced ergogenic effect of caffeine and may need to consume more caffeine for any ergogenic benefit while those with a CYP1A2-AA genotype need less caffeine and experience more benefits than those with the C subtype.[14]
This finding supports common sense: we are only discussing general ideas — pick the dose that best fits your needs. If 5mg/kg makes you feel you’re about to die, you should lower your dose.
Overcoming Caveats
Because we’re PricePlow, we have to cover how an individual can make caffeine more efficiently. The best answer is an idea that none of us want to hear - dose caffeine less often. Current data suggests that athletes can use caffeine daily until tolerance develops around the 15-18 days mark.[17] The athletically minded amongst us may recognize that 15-18 days is perfect for closing out an intensity block or realization period in strength training. Therefore, our first recommendation is to save caffeine for periods where you really want it to work its best. While even writing this shocks and offends the PricePlow staff, the benefits of quitting caffeine for short periods of time may lead to better gains through deepened sleep quality.[18]
Does this feel familiar to you?[18] Sometimes we need strategies to avoid this 'downward spiral'
Another approach is to halve your caffeine intake a few days per week — an approach suggested by Joseph Rivera, a “coffee researcher” that created a website called Coffee Chemistry.[19] While we had difficulty backing up this approach with cold-hard exact studies showing a benefit to this technique — it makes sense that halving a dose would be proficient for lowering tolerance at least slightly. If you’re a PricePlow reader, you are statistically a massive consumer of caffeine — so this may be an ideal approach if quitting everyone’s favorite mixed xanthine is unfathomable.
Now that everyone hates us for suggesting you quit caffeine to enjoy caffeine, we’ll cover a method that don’t involve lower doses. Caffeine metabolizes within an hour of ingestion. Therefore, it is likely prudent to consume your caffeine dose via a bolus an hour before you need to perform at your best.[20]
The source of caffeine is up to individual choice. One paper in 1998 showed that caffeine and water outperformed other sources of caffeine, including coffee, despite an equal dose of caffeine across all research subjects.[21] While some papers refute this point, coffee can be a great ergogenic aid as long as you aren’t stuck in the bathroom the whole workout.[22]
Synergism: Why Pre-Workouts Hit Different
Caffeine appears to act synergistically with other pre-workout ingredients. We all know that L-Theanine can reduce the jitters and anxiety lifters may experience with high caffeine doses. This combo is a well-researched duo even in humans models.
If chasing caffeine-based performance, it appears prudent to keep caffeine doses between 4-7mg/kg of bodyweight per day
L-tyrosine may also be an interesting addition to a caffeine bolus. As mentioned previously, caffeine encourages the release of catecholamines. L-tyrosine is a precursor of many neurotransmitters, so having more L-tyrosine around may encourage the body to make more catecholamines. The catecholamines mediate the body’s “fight or flight” response — which may help improve caffeine’s “ready for war” effect.[23] This combination has not been studied much and is mostly postulation.
Theacrine is an interesting addition that gives caffeine some “parallel” help. Like caffeine, theacrine is a mixed xanthine compound with stimulant effects However, it does not appear to be subject to the rapid tolerance induction that bars caffeine from being the best stimulant around.[24] It also takes nearly an hour longer to metabolize.[25] Better yet, mixing caffeine and Theacrine is a new research hot bed, so we hope to have more to come in the future on that.[26] Therefore, theacrine offers a “parallel” stimulant to caffeine that lasts longer while also being tolerance resistant. However, it tastes absolutely terrible and needs care in its masking by supplement formulators and flavorists.
Concluding Statements
We hope you've enjoyed this article! Leave comments via the PricePlow Forum below!
If chasing caffeine-based performance, it appears prudent to keep caffeine doses between 4-7mg/kg of bodyweight per day to avoid side effects — which can be fatal. Caffeine tolerance accumulates within 14-18 days — but lifters can combat this by taking a few weeks off or by intermittently halving their intake. It is best to take caffeine about an hour before a performance-demanding event. If you want to stack caffeine with other ingredients —l-theanine, l-tyrosine, and theacrine are places to start. Like all things, exhibit common sense and find what works for you! Use guidelines to guide yourself to the dose and timing that best suits your needs as an athlete.
We hope you now realize that companies recommending “2-3” scoops of a product are just trying to get you to run of tubs more frequently. Label recommendations are not your friend - educate yourself in this golden era of awareness and buy products that fit the clinically studied doses. Then again, if you trust companies with your health...maybe dive more into our other guides available on our supplement guides page.
Pre Workout Supplements – Deals and Price Drop Alerts
Get Price Alerts
No spam, no scams.
Disclosure: PricePlow relies on pricing from stores with which we have a business relationship. We work hard to keep pricing current, but you may find a better offer.
Posts are sponsored in part by the retailers and/or brands listed on this page.

Comments and Discussion (Powered by the PricePlow Forum)