
When a label says "folate," you'd assume you're getting what your body actually uses. Often you're not. Balchem's Optifolin+ delivers active 5-MTHF folate directly, and a 2025 trial found it absorbs 2.6x better than folic acid.
When consumers read "folate" on a label, they typically assume they're getting the nutrient their body actually uses. In reality, the answer depends heavily on the form. Most supplements still rely on folic acid, a synthetic precursor that must be converted before it becomes biologically active. For some people, that conversion happens efficiently. For others, it may not.
Folate and the Form Problem Nobody Talks About
The answer depends heavily on the individual. Folic acid is a synthetic, oxidized compound the body can't use directly, and is rarely found in nature. It requires multiple enzymatic conversion steps to reach the active state your cells actually need. Genetic variations in folate metabolism enzymes, including MTHFR variants that are common up to 40% of the population,[1] may further reduce the efficiency of converting folic acid to active folate forms. The gap between the dose on a label and the folate the body actually receives can be wider than most consumers or formulators realize.
Introducing Optifolin+: Balchem’s Enhanced Science-Backed Folate Source
Optifolin+ is Balchem's solution to this problem. It's a choline-enriched, (6S)-5-methyltetrahydrofolate (5-MTHF), the naturally occurring form of folate found in human blood, it enters circulation without requiring any conversion steps, doesn't produce unmetabolized folic acid in the bloodstream, and according to Balchem's data, it carries a 7x methyl agent advantage over other leading folate forms. A 2025 randomized controlled trial found it absorbed 2.6x more efficiently than folic acid, reaching peak folate concentration 3.5x faster.[2]
Below, we get into the science of Optifolin+, why folate form matters, and what a bioactive form solves that synthetic folic acid can't. Stay up to date on Optifolin+ and new products as they come to market:
Subscribe to PricePlow's Newsletter and Optifolin+ Alerts
Folate’s Role in the Body
Folate (vitamin B9) sits at the center of two of the body's most fundamental processes: DNA synthesis and methylation.[3]
Every round of cell division requires folate to accurately replicate the genetic code. During periods of rapid cell turnover (fetal development most critically), demand spikes considerably. The neural tube, which becomes the brain and spinal cord, closes between days 21 and 28 after conception, often before a woman even realizes she's pregnant. That timing gap is why pre-conception folate status matters as much as supplementation during pregnancy itself.[4]
Beyond DNA, folate drives one-carbon (C1) metabolism: the biochemical network that generates S-adenosylmethionine (SAM), the body's universal methyl donor. SAM fuels a wide range of methyltransferase reactions involved in neurotransmitter synthesis, gene expression, epigenetic regulation, and protein metabolism. Folate also powers homocysteine remethylation through the methionine synthase (MS) pathway, converting homocysteine back to methionine and supporting healthy cardiovascular function.[5]
Even with mandatory folic acid fortification, a meaningful share of US adults fall short of the 400mcg DFE RDA,[3] and the supplement form chosen matters more than it's often given credit for.
Why Folic Acid Falls Short
To become metabolically active, folic acid must be reduced to dihydrofolate by the enzyme dihydrofolate reductase (DHFR), then converted further through 5,10-methylenetetrahydrofolate to reach the usable end form: 5-methyltetrahydrofolate (5-MTHF). Importantly, 5-MTHF is the primary folate species normally found in human blood.[6] This means there are three steps governed by multiple enzymes, with real bottlenecks introduced at each stage.
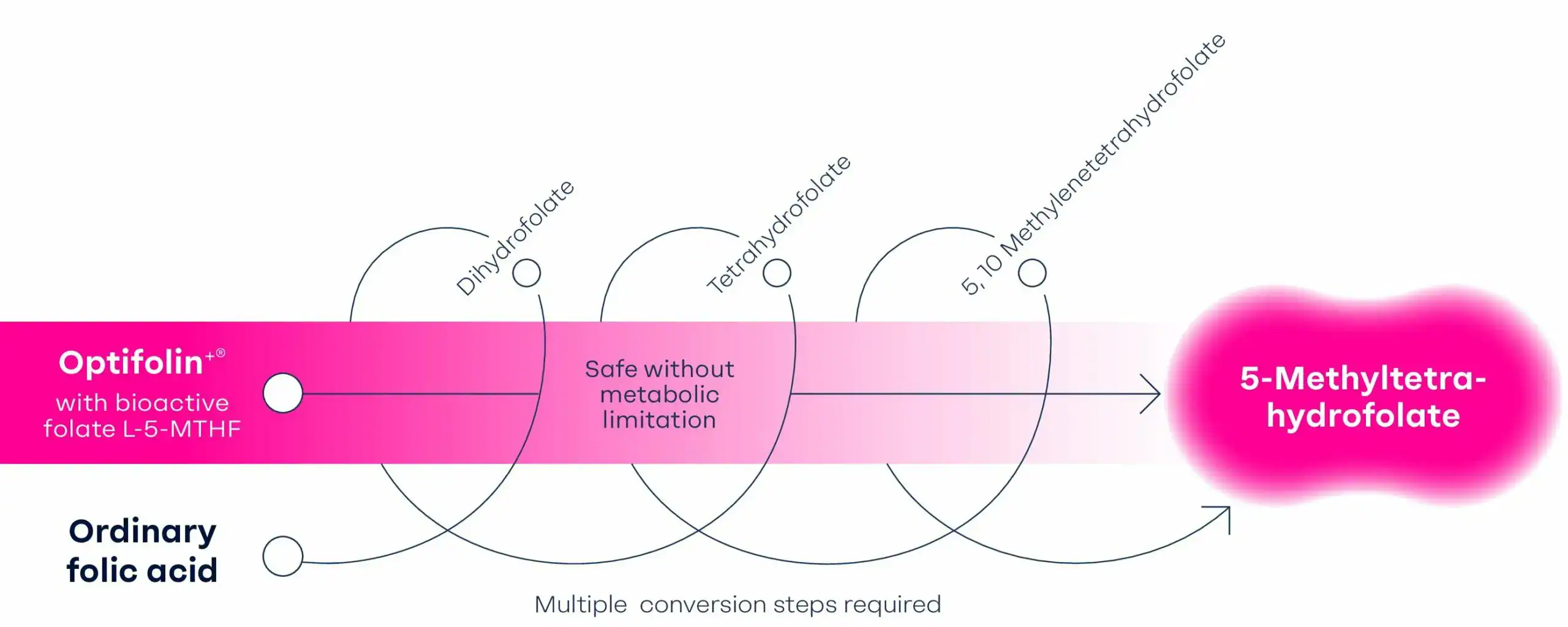
Optifolin+ enters the body as bioactive L-5-MTHF and reaches the active folate form without metabolic limitation, while ordinary folic acid has to clear several enzyme conversion steps first.
-
Problem 1: The DHFR Bottleneck
Bailey and Ayling measured DHFR activity in human liver samples and found it ran at less than 2% the rate of rat liver at physiological pH, with nearly five-fold variation across the six human samples tested.[7] Most early folate research used rodent conversion rates as the baseline, but those substantially overestimate what human liver can actually do. This means higher folic acid doses saturate the conversion pathway rather than producing proportionally more active folate.
-
Problem 2: MTHFR Polymorphisms
The methylenetetrahydrofolate reductase (MTHFR) enzyme handles the final conversion step to 5-MTHF. The common C677T genetic variant reduces MTHFR activity, limiting how much active folate the body can generate from a given folic acid dose. Up to 40% of people in some populations carry at least one copy of this variant, with prevalence varying considerably by geographic region and ethnicity.[8,9] For those individuals, reduced MTHFR activity compounds the already-limited DHFR bottleneck.
-
Problem 3: Unmetabolized Folic Acid in Circulation
When folic acid intake exceeds conversion capacity, unmetabolized folic acid (UMFA) appears in the bloodstream. Kelly et al. found a threshold around 200mcg per dose: above that amount, folic acid appeared unaltered in serum.[10] A standard 400mcg daily dose (widely recommended for pregnancy support) clears that threshold in a single serving.

Circulating UMFA has been associated with potential downstream effects. Troen et al. detected UMFA in 78% of fasting plasma samples from a cohort of 105 postmenopausal women and found an inverse relationship with natural killer (NK) cell cytotoxicity: NK cell activity was approximately 23% lower in women with detectable UMFA, with the relationship strengthening at higher concentrations.[11] These findings are specific to postmenopausal women, and more research is needed before drawing broader conclusions, but they add to the practical case for a folate form that enters circulation directly as L-5-MTHF.
High-dose folic acid also carries a well-documented masking concern: it can normalize the hematological signs of vitamin B12 deficiency while potential underlying neurological damage continues undetected.[6] L-5-MTHF is generally considered less likely to mask vitamin B12 deficiency because it is the biologically active circulating form of folate.
Optifolin+: Choline-Enriched Bioactive Folate for Supplement Brands
Optifolin+ is a choline-enriched (6S)-5-methyltetrahydrofolate: the naturally-occurring, physiologically active form of folate paired with two choline molecules. Because it's already 5-MTHF, it enters circulation without any DHFR or MTHFR enzyme dependency. It is without conversion bottleneck, UMFA generation, or sensitivity to the five-fold individual variation in DHFR activity.
Why Choline Is the Right Salt for Broader Consumer Acceptance
Most L-5-MTHF products use calcium or glucosamine as their counterion. Optifolin+'s use of choline is both functionally significant and a sound chemistry decision.
Tom Druke, Senior Marketing Manager at Balchem, breaks down the science of VitaCholine®, Albion® chelated minerals, and K2VITAL® on Episode #216 of the PricePlow Podcast. Plus: the story behind Balchem's first-of-its-kind New York Jets ingredient partnership.
Choline is an essential methyl donor that fuels the betaine homocysteine methyltransferase (BHMT) pathway, which operates independently of the folate-dependent methionine synthase route. The BHMT pathway accounts for approximately 50% of cellular SAM production under normal conditions.[5] The two pathways are also metabolically interdependent: in rodent models, choline-deficient diets reduce liver folate by 31% to 40%, and folate deficiency depletes hepatic choline stores in turn.[5] By combining both in a single compound, Optifolin+ supports methylation through two complementary routes simultaneously.
According to Balchem's data, this structure gives Optifolin+ a 7x methyl agent advantage over other leading folate forms and 98% active methylating capacity.[5] Balchem is also well-known for their expertise in choline, thanks to VitaCholine®, their branded and research-backed choline. .
Formulation Flexibility
L-5-MTHF is notoriously unstable in some salt forms. Balchem's internal comparative benchmark data shows that Optifolin+ maintains full label-claim potency across its 36-month shelf life at 25°C/60% relative humidity. In Balchem's internal comparative testing, Optifolin+ maintained potency across its labeled shelf life, while comparator methylfolate salts showed greater degradation under the same conditions. A product that loses active ingredient before a consumer opens the bottle isn't delivering its label claim, and brings risk to brands that are using it.
Optifolin+'s water solubility (1:1 parts solute to solvent) also gives it a broader application range. The choline salt is stable in capsules, tablets, and gummies, and soluble enough for softgels, droppers, and liquid formats, bringing a flexibility that calcium-based 5-MTHF salts can't match in aqueous applications.
The Absorption Data: Optifolin+ vs. Folic Acid
![]()
The landmark clinical study on Optifolin+ is a 2025 randomized, double-blind, crossover pharmacokinetics trial published in Food & Nutrition Research. Twenty-four healthy adults (ages 29 to 40, male and female) received a single equimolar oral dose of either 400mcg folic acid or 603mcg Optifolin+, with a 14-day washout between treatments. Researchers tracked total folate and 5-MTHF pharmacokinetics over 24 hours, including area under the curve, peak concentration, time to peak, and unmetabolized folic acid levels.[2]
Optifolin+ outperformed folic acid on every measured endpoint:[2]
- 5-MTHF iAUC(0-8h) was 2.56x higher with Optifolin+ (p<0.0001)
- Time to peak 5-MTHF concentration was 3.5x faster (p<0.01)
- UMFA levels showed no measurable increase after Optifolin+, while folic acid produced a significant UMFA spike peaking around 1 hour and remaining detectable at 1.5 hours (p<0.01 vs. baseline)
The bioavailability advantage held in both sexes: 5-MTHF iAUC was 2.1x higher in women and 3.1x higher in men compared to folic acid. The researchers attributed part of the absorption advantage to Optifolin+'s high water solubility (650mg/mL under neutral conditions), which facilitates efficient gut absorption independently of the enzymatic barriers that limit folic acid.[2]
Improved Label Credibility
The adult RDA for folate is 400mcg DFE daily, rising to 600mcg DFE during pregnancy and 500mcg DFE while lactating. No tolerable upper intake level has been established for L-5-MTHF, in contrast to folic acid's 1mg/day UL set by the Institute of Medicine. This reflects on the fact that 5-MTHF is the body's native circulating form rather than a synthetic precursor requiring conversion.[12] It doesn't mask vitamin B12 deficiency, and it doesn't generate UMFA at standard doses.

For labeling, Balchem recommends a conservative 1:1 DFE-to-Optifolin+ conversion (400 micrograms DFE = 400 micrograms Optifolin+). FDA guidance allows manufacturers of synthetic folates such as L-5-MTHF to use their own established conversion factors, provided the declaration is truthful and not misleading, and FDA states it would not expect the conversion factor to exceed 1.7, comparable to folic acid.[13]
Supplement facts panels should list Optifolin+ as: "Folate (as 6(S)-5-methyltetrahydrofolate as Optifolin+®)." Optifolin+ has received a New Dietary Ingredient Notification (NDIN) in the US[14,15] and is manufactured to US and EU cGMP standards (PIC/S, ICH Q7, and ICH Q10). It's Kosher, Halal, and allergen-free.
Form Is the Foundation
The supplement industry has relied on folic acid for decades, largely because it's stable, inexpensive, and meets the label requirement. But when the conversion pathway has a hard ceiling, varies five-fold across individuals, and gets further compromised in a meaningful share of the population, the label doesn't tell the whole story.
Optifolin+ addresses the form problem directly and intelligently. It delivers folate as the active species the body actually uses, pairs it with a choline counterion that contributes independently to the methylation cycle, and now has a 2025 RCT confirming clear bioavailability and absorption advantages over folic acid.
Interest in methylation, personalized nutrition, cognitive health, and prenatal wellness has increased demand for more bioavailable forms of B vitamins. As a result, formulators are increasingly evaluating whether the traditional folic acid approach still represents the optimal solution.
Folate has long been considered a solved category. Yet growing research around bioactive folate, methylation biology, and nutrient utilization suggests there may still be room for meaningful innovation.
Comments and Discussion (Powered by the PricePlow Forum)